

AI All Over
AI All Over
DCMedical News is published every day both the House and the Senate are scheduled to be in session.
DCMedical News is supported by readers like you. Click here for an optional paid subscription.
In Cancer Treatment
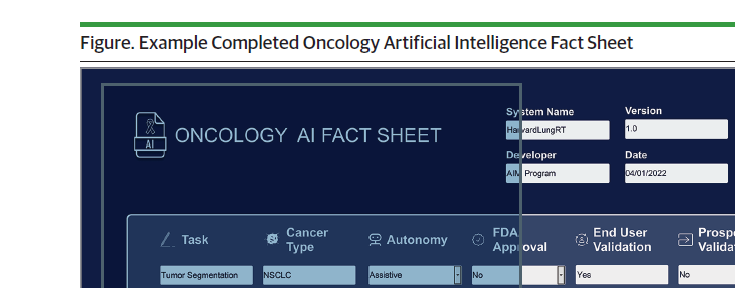
Researchers publish an “A.I. Fact Sheet” for cancer clinicians and researchers, in JAMA Oncology (here), for the “safe use and ethical deployment” of AI in cancer care. They note, “Artificial intelligence (AI) systems—which consist of an AI algorithm and the contexts in which it is deployed—are increasingly obtaining US Food and Drug Administration (FDA) approval and entering the oncology clinic. Artificial intelligence can now assist with fundamental steps of cancer care, including cancer screening, clinical risk prediction, and radiotherapy planning. But especially in early days of implementation, there are risks associated with inappropriate AI use, as well as unknown effects of human factors on system performance in the clinic.”
In Physician Notes
And MedPage Today reports that “Early adopters say generative AI can now be used to write physician notes and patient-facing text like disease summaries.” The clinical note writing app, powered by GPT4 (here), will be released this year by Nuance and Microsoft. “Known as Dragon Ambient eXperience (DAX) Express, [it] will be able to create an automatic clinical note based on recordings of patient visits.”
“DAX Express will combine ambient and conversational sound recordings with the generative AI capabilities of GPT-4 to capture and analyze patient encounters with their provider and produce a draft of a standardized clinical note for the provider's review. The recording will be captured using the provider's mobile device. The whole process is supposed to take a few seconds after each patient visit, and it will allow the provider to focus on the patient while still having final sign-off on the documentation.”
MedPage reports that “However, not everyone in the healthcare industry is completely convinced that adding an AI-powered application will be the salve to the issues of provider burnout. A recent survey by the Pew Research Center revealed that fewer than half of Americans believe that AI can improve patient outcomes, and 60% said they would feel uncomfortable if their provider relied on it for medical care.”
“The earlier model of this AI-powered automatic documentation application . . . notably included an additional reviewer working behind the scenes to prepare the draft clinical note for a provider's review. A senior executive at Nuance acknowledged in the article that trusting AI can be challenging in part because of its proclivity to ‘hallucinate,’ a term coined to describe the confident falsehoods frequently produced by AI chatbots, like ChatGPT.”
“The current DAX application still takes up to 4 hours to generate each clinical note because it requires a human reviewer, so the potential of the new GPT-4-powered application to instantly draft each note could be the thing that changes how healthcare providers view this technology.”
“The application will be made available to a select group of Nuance's clients during the summer for a private preview, then the company will fully release the application in the fall . . . Nuance currently has more than 550,000 providers using its current Dragon applications.”
And in Coding
And the AMA notes (here, in “AI Taxonomy Enables Future Health Care Innovation,” in the AMA’s CPT Quarterly) what will undoubtedly be an important path for AI application, coding.
HOSPITALS, NURSING HOMES AND OTHER HEALTH CARE FACILITIES
KHN on Medical Debt
The Kaiser Health Network reports (here) on medical debt, finding that “Around 100 million Americans have health care debt, and together they owe at least $140 billion. And research suggests this debt can have striking consequences on people’s financial, physical, and mental health . . . More than half say they’ve had to make a difficult sacrifice, like using up all their savings, moving in with friends and family, or losing their homes. So, I don’t think it’s hyperbole to say that there’s a shocking amount of misery out there.”
Large Non-Profit Health Systems Lost Money in the Market in 2022
Researchers supported by Arnold Ventures and publishing in Health Affairs (here) discover that health system net income includes non-operating income, and, based on analysis of a quarterly report from 10 such systems, argue that federal dollars should not be used to bail out market gambling.
“If losses were driven by persistent labor and supply cost increases, then it might be reasonable to ask patients, employers, and insurers to consider these underlying cost drivers in their payments to hospitals. However, when losses are driven by risky financial investments, which generated positive returns in many previous years and will do so in many future periods, it is not clear whether patients, employers, insurers, and taxpayers should be responsible for paying higher prices to offset the impact of overall market declines.”
MEDICARE, MEDICAID, AND COMMERCIAL HEALTH INSURANCE
ProPublica Reports on “How Cigna Saves Millions by Having its Doctors Reject Claims Without Reading Them.”
A rejected claim led a suspicious patient (who happened to be a doctor) covered by a Cigna policy to inquire further. A report on the patient’s claim and a subsequent investigation by ProPublica (here) notes that “The rejection of [the patient] claim was typical for Cigna, one of the country’s largest insurers.”
“The company has built a system that allows its doctors to instantly reject a claim on medical grounds without opening the patient file, leaving people with unexpected bills, according to corporate documents and interviews with former Cigna officials. Over a period of two months last year, Cigna doctors denied over 300,000 requests for payments using this method, spending an average of 1.2 seconds on each case, the documents show. The company has reported it covers or administers health care plans for 18 million people.”
“Medical directors do not see any patient records or put their medical judgment to use, said former company employees familiar with the system. Instead, a computer does the work. A Cigna algorithm flags mismatches between diagnoses and what the company considers acceptable tests and procedures for those ailments. Company doctors then sign off on the denials in batches, according to interviews with former employees who spoke on condition of anonymity.”
“We thought it might fall into a legal gray zone,” said the former CIGNA official, who helped conceive the program. “We sent the idea to legal, and they sent it back saying it was OK.”
The system, however, is unlike “prior authorization.” The story reports “Cigna emphasized that its system does not prevent a patient from receiving care — it only decides when the insurer won’t pay.”
“Cigna eventually designated the list PXDX — corporate shorthand for procedure-to-diagnosis. The list saved money in two ways. It allowed Cigna to begin turning down claims that it had once paid. And it made it cheaper to turn down claims, because the company’s doctors never had to open a file or conduct any in-depth review. They simply denied the claims in bulk with an electronic signature.”
PUBLICATION SCHEDULE FOR DCMEDICAL NEWS
March 28, 29, 30
April 17, 18, 19, 20, 25, 26, 27, 28
May 9, 10, 11, 12, 15, 16, 17, 18
Notes to Fred Hyde, MD, JD, MBA, news@dcmedicalnews.org
© 2023 Fred Hyde & Associates, All rights reserved.
Editor: Jane Guillette; Systems and Distribution: Colby Miers, Los Angeles