

Medicare Fight Heats Up: Are Proposed Limits on Benefits, or on Fraud?
Medicare Fight Heats Up: Are Proposed Limits on Benefits, or on Fraud?
DCMedical News is published every day both the House and the Senate are scheduled to be in session.
The political opponents are clear. One side says fighting fraud will help “right the ship” financially for Medicare. The other says that “fraud fighting,” especially when Medicare Advantage plans are suspected of the fraud, will deprive MA beneficiaries of benefits.
The Washington Post (here) checks in, contending that “A fiscally responsible government cannot keep its hands off Medicare.” Reports The Post, “During fiscal 2022, the program accounted for $710 billion in federal spending, which was 11.4 percent of the $6.2 trillion total [federal government spending] . . . By 2028, the Medicare trust fund, which pays for hospitals, skilled nursing facilities and hospices, and is financed by payroll taxes, is expected to be exhausted. No rational approach to fiscal sustainability could wall off so many of the dollars that Washington spends every year.”
“To be sure, President Biden proposed, in his 2024 budget, changes that would keep Medicare solvent for 25 years. He would accomplish this by adding more drug price negotiations (on top of the ones in last year’s Inflation Reduction Act) and raising a tax on the investment income of people who earn more than $400,000 a year. The president deserves credit at least for discussing the topic, but his plan is mostly political messaging rather than a serious approach to the issue. It places the entire burden of ensuring Medicare solvency on unpopular drug companies and high-income earners, implying — incorrectly — that structural reforms are unnecessary.”
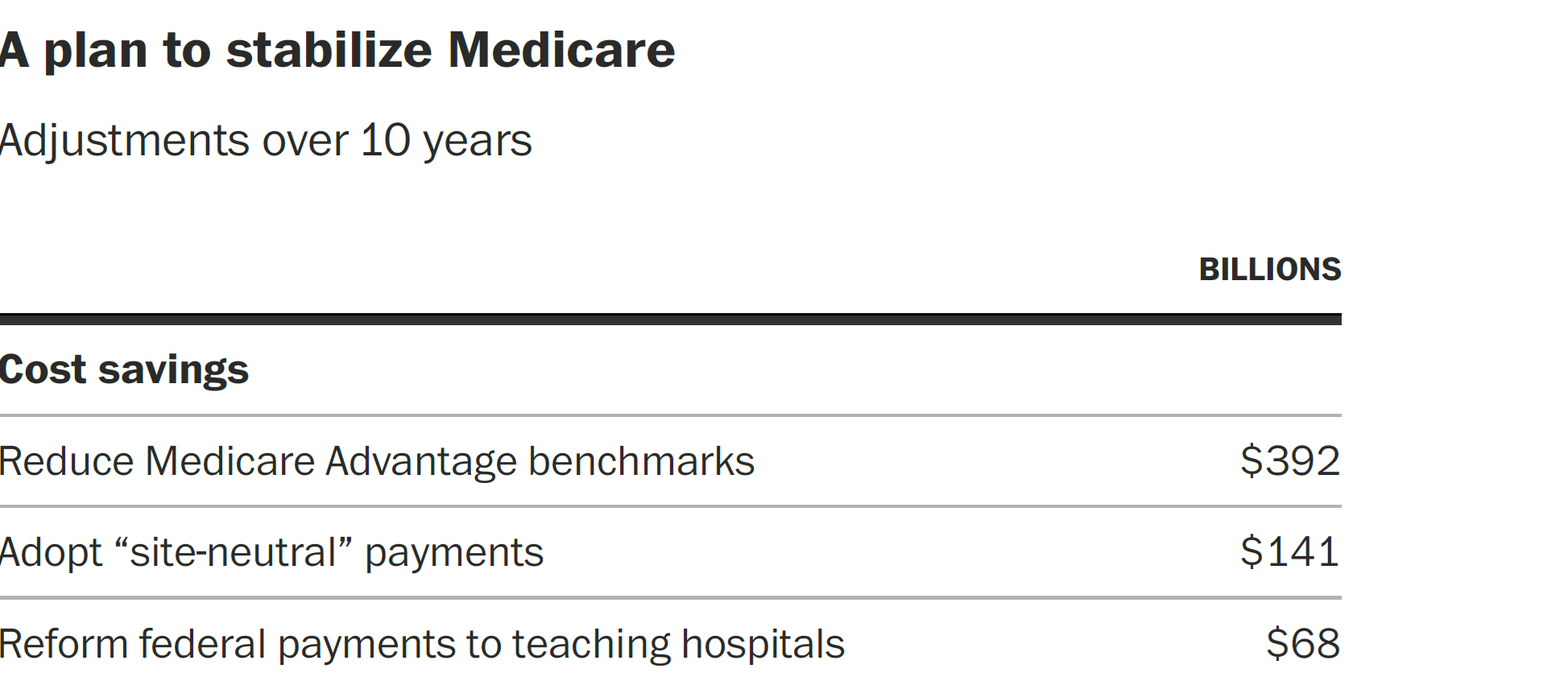
The “structural reforms” advocated by The Post include limiting extra pay to Medicare Advantage (MA) plans by limiting upcoding, and elimination of the site-of-service differential.
“Containing costs for Medicare Advantage, the alternative to traditional fee-for-service Medicare that now covers roughly half of all beneficiaries, is probably the most important step the president and Congress could take . . . the program costs more per beneficiary than traditional Medicare — 4 percent more, according to the latest government data. This is in part the perverse result of upward rate adjustments the government awards insurers to cover patients with higher risk scores, which incentivize Medicare Advantage companies to maximize each client’s reported ailments (known as upcoding). These adjustments, in turn, are made to rates that companies and the government negotiate relative to a predetermined baseline. Reducing that so-called benchmark by 10 percent would save the taxpayers a whopping $392 billion over 10 years, according to the CBO.”
On site-of-service, The Post notes “Medicare pays more for services performed on an outpatient basis at hospitals than it does for the same services done at physicians’ offices or ambulatory surgical centers. This makes no sense and creates an incentive for hospitals to buy up independent doctors’ offices that they then relabel as hospital facilities. Eliminating this discrepancy could save $141 billion over 10 years. Equally irrational are the different co-pays and deductibles traditional Medicare assesses for doctor visits and hospital stays. Replacing that system with uniform cost-sharing rates and an annual out-of-pocket cap would save $27 billion over 10 years.”
Other targets: how Medicare pays for medical education, and how it offsets hospital bad debts.
The New York Times weighs in (here), also on the side of “reforming” Medicare Advantage. The Times reports on massive advertising on the subject, including a Super Bowl ad on behalf of preserving the MA plan extra payments. Reports The Times, “Their conversation in a Super Bowl ad focused on a Biden administration proposal that one bowler warned another would cut Medicare Advantage . . . The multimillion-dollar ad buy is part of an aggressive campaign by the health insurance industry and its allies to stop the Biden proposal. It would significantly lower payments — by billions of dollars a year — to Medicare Advantage . . . The change in payment formulas is an effort, Biden administration officials say, to tackle widespread abuses and fraud in the increasingly popular private program. In the last decade, reams of evidence uncovered in lawsuits and audits revealed systematic overbilling of the government. A final decision on the payments is expected shortly, and is one of a series of tough new rules aimed at reining in the industry. The changes fit into a broader effort by the White House to shore up the Medicare trust fund.”
The Times added, “Some Medicare Advantage plans from UnitedHealth reported that half of their patients had vascular disease, in contrast with just 14 percent in the basic government program. UnitedHealth said the study highlighted how its plans provided better care . . . In its lawsuit against Cigna last October, for example, the Justice Department described an insurance executive’s email that referred to diabetes with complications; depression; and vascular disease as the ‘golden nuggets we are looking for.’”
Other voices contend that control over MA excesses will promote inequity, or will disadvantage dual eligible patients (here). An editorial in The Hill (here) says “If the government cut Medicare fraud, it wouldn’t have to cut Medicare.”
DOCTORS, NURSES, AND OTHER HEALTH PROFESSIONALS
Large Thrombectomy Trial Halted, Benefit Demonstrated
In “Benefits of Stroke Thrombectomy Extend to Patients with a Large Core Infarct” researchers (editorial here, research here) report that “Two multicenter randomized trials were stopped early after demonstrating clear benefits of stroke thrombectomy in patients with larger strokes” (approximately 20% of all strokes). They noted, “Thrombectomy represents one of the most effective treatments in medicine: the number needed to treat to prevent disability in one patient with stroke is 2.3 . . . The improved chance of independent walking and the ability to perform other daily activities in patients with the most severe strokes is welcome news for patients and for the field of stroke treatment.”
HOSPITALS, NURSING HOMES AND OTHER HEALTH CARE FACILITIES
Imperfect Markets
Jaime King reports (here in NEJM) “On Consolidation and Competition — The Trials and Triumphs of Health Care Antitrust Law.” She writes, “Over the past 30 years, health care consolidation has gone largely unchecked by federal and state antitrust enforcers, which has resulted in higher prices, stagnant quality of care, and limited access to care for patients. Similarly, consolidation has contributed to the availability of fewer employment options, limited wage growth, longer hours, and staff shortages for health care providers. Antitrust law is designed to prevent such harms,
but its failure to evolve alongside the health care industry has led to pervasive consolidation, which now necessitates regulation in some markets to address market power abuses that competitive forces can no longer govern.” Her anti-trust time-line history map follows the Sherman Act (1890) through FTC v. Hackensack Meridian Health (2022).
You Can Say That Again, and Again
In JAMA Internal Medicine a viewpoint (here) notes that the multiple, many-fold communications of large health systems to actual or prospective patients could “devolve into a cacophony of excessive, intrusive, and irrelevant messages.”
“Large, integrated health care systems, such as the US Department of Veterans Affairs and Kaiser Permanente, are expanding their communication portfolio to include system-generated appointment reminders from primary care and multiple specialty clinics, prompts to complete laboratory and imaging tests, medication reminders from system pharmacies, surveys to assess satisfaction with care, billing notices, and population health messages to encourage healthy lifestyles and disease-prevention practices.”
“Because individual communication campaigns may be effective, health care systems can be tempted to pile on
messages without considering the overall volume or content messages the patient receives. If patients begin to feel that these campaigns are not well coordinated or that certain messages are unnecessary, impersonal, or repetitive, then they may start to ignore them, regardless of content.”
PUBLICATION SCHEDULE FOR DCMEDICAL NEWS
March 29, 30
April 17, 18, 19, 20, 25, 26, 27, 28
May 9, 10, 11, 12, 15, 16, 17, 18
Notes to Fred Hyde, MD, JD, MBA, news@dcmedicalnews.org
© 2023 Fred Hyde & Associates, All rights reserved.
Editor: Jane Guillette; Systems and Distribution: Colby Miers, Los Angeles