

Tax Exemption for Hospitals Scrutinized by GAO
Tax Exemption for Hospitals Scrutinized by GAO
DCMedical News is published every day both the House and the Senate are scheduled to be in session.
Click here to support DCMedical News.
The General Accountability Office testified before a House Subcommittee Wednesday (press release here, one page report summary here, full report from the GAO here) that the IRS has insufficient guidance from Congress to ensure that tax exempt hospitals operate in a manner which would justify their tax exempt status.
“In September 2020, GAO recommended Congress consider specifying what services and activities demonstrate sufficient community benefit. As of April 2023, Congress had not enacted such legislation. GAO also recommended IRS update tax forms to increase transparency about hospitals' community benefits. IRS agreed and made minor adjustments to the form's instructions, but the form still relies on a narrative description of community benefits that hospitals provide.”
The IRS presentation of its new report took place before the Subcommittee on Oversight of the House Committee on Ways and Means. The report summarized the organization, community benefit and PPACA-based requirements for tax exemption, as follows:
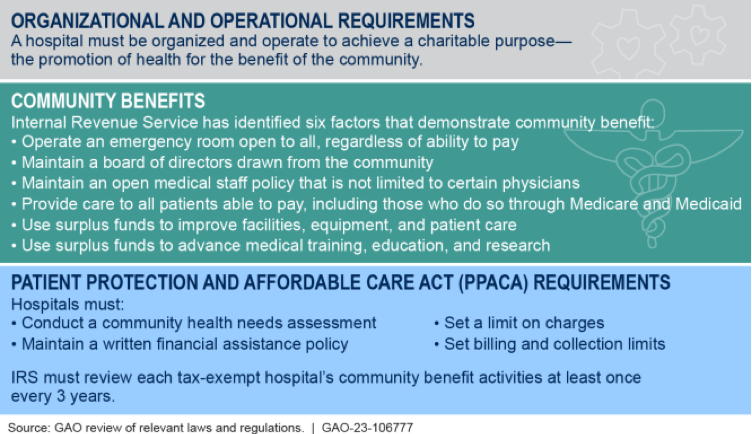
The report explains, the “IRS does not have authority to specify activities hospitals must undertake and makes determinations based on facts and circumstances. As a result, tax-exempt hospitals have broad latitude to determine the community benefits they provide, but the lack of clarity creates challenges for IRS in administering tax law.”
Board Financial Assistance
Embarrassingly, at least its timing, is a new report (here) on non-profit hospitals that pay board members for their service. Findings: “Among all nonprofit hospitals, more than 37 percent compensated their board members in 2019. From 2011 to 2019, nonprofit hospitals that paid board members increased compensation by 57 percent, rising from $31,964 to $50,156 . . . On average, a $10,000 increase in average board member compensation was linked with a nearly $70,000 decrease in annual provided charity care. From 2011 to 2019, the average charity care-to-expense ratio for nonprofit hospitals that paid board members decreased from 2.5 percent to 1.6 percent.”
HOSPITALS, NURSING HOMES AND OTHER HEALTH CARE FACILITIES
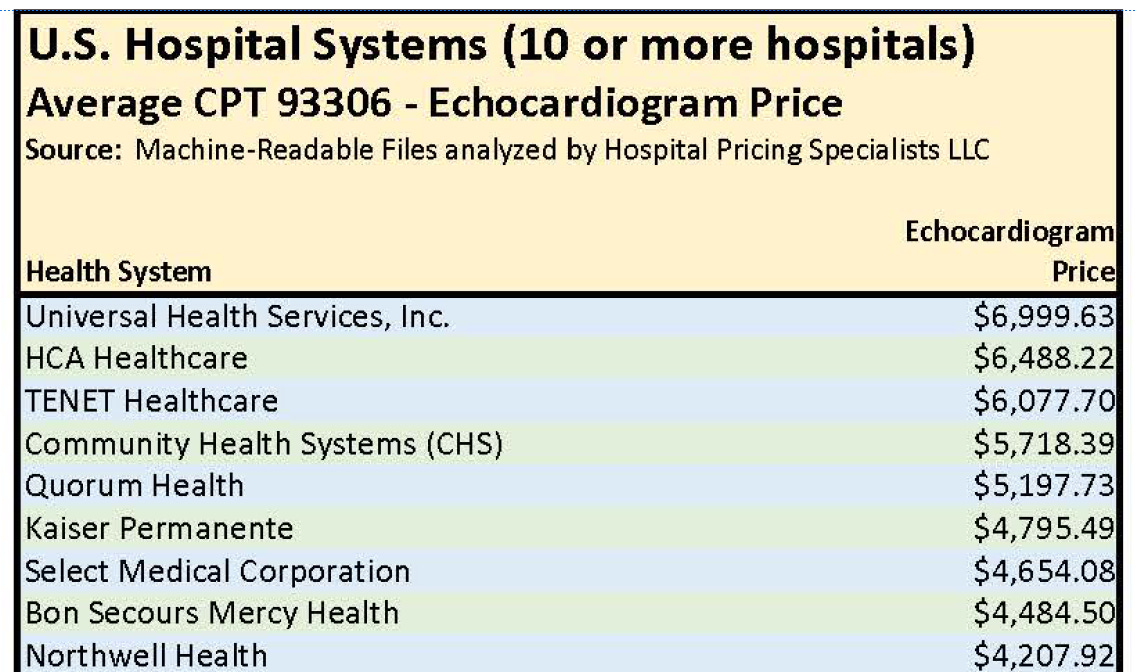
How Much for that Echocardiogram? Maybe $6,999? Maybe $78.10?
Rick Louie, whose Hospital Pricing Specialists issues periodic reports based on hospital charges or list prices, has published his third annual collection of such prices for echocardiograms. His study found, in “analyzing the machine-readable files of 4,231 hospitals in the US . . . with increased price transparency, the coefficient of variation (CV) has tightened from the prior year.”
His database (here) shows the highest price to be $19,375 (two hospitals in New Jersey). The lowest price, $78.10, is a hospital in Maryland. No doubt due to the “all payer” state-controlled system, the six lowest charges and half of the lowest 25 charges nationally are from Maryland hospitals.
“Unified” Post Acute Payment System Proposed to Congress by MedPAC
The Medicare Payment Advisory Commission has now sent to Congress a proposal (report here) which would cover all four post-acute care settings for which the Medicare program makes payments. The four -- home health agencies, skilled nursing facilities, long-term care hospitals and inpatient rehab facilities -- have different mechanisms for payment now, but the recommended change “should base payments off patient characteristics, rather than the setting.” MedPAC was responding to a near decade old Congressional directive to make such a report, and some MedPAC Commissioners immediately expressed doubt about the means of implementation and the potential for “gaming” (treating the risk adjustment rather than the riskier patient, in the manner of Medicare Advantage Plans).
Modern Healthcare reported (here) some rationale for the move, “The separate payment plans not only make the quality measures and patient assessments difficult to compare but, before the recent updates to the setting-specific prospective payment systems, also gave way for long-term care hospitals to admit more patients with less severe or complex conditions and incentivized nursing homes and rehab facilities to push unnecessary therapies.”
DRUGS & DEVICES
Are Pharmacy Benefit Managers Gangsters?
Ohio’s Attorney General thinks so. “PBMs are modern gangsters,” Attorney General Yost said. “They were designed to protect and negotiate on behalf of employers and consumers after Big Pharma was criticized for overpricing medications, but instead they have absolutely destroyed transparency, scheming in the shadows to control drug prices on all sides of the market.” So, he filed suit (here).
“This collusion has been made possible by PBM market consolidation, which has left the three largest PBMs, including Express Scripts, in control of more than 75% of the drug market and the three next largest in control of much of the rest.”
“In marketing its services, Express Scripts touts its ability to leverage its significant market power to extract lower drug prices from drug manufacturers and promises to deliver cost savings to health insurers and employers – a promise that is knowingly false . . . Rather, Express Scripts has used its dominance solely for its own financial gain, creating “a complex ‘pay to play’ rebate system that, perversely, pushes manufacturers to increase drug prices in order to be placed on, or receive, preferred placement on PBM formularies. The savings that PBMs claim from the inflated list prices are illusory.”
The AG’s Complaint begins, “Like the importation of kudzu to stop soil erosion, the creation of the pharmacy benefit manager was a solution that has become the problem.”
PUBLICATION SCHEDULE FOR DCMEDICAL NEWS
April 28
May 9, 10, 11, 12, 15, 16, 17, 18
June 6, 7, 8, 11, 12, 13, 14, 20, 21, 22, 23
Notes to Fred Hyde, MD, JD, MBA, news@dcmedicalnews.org
© 2023 Fred Hyde & Associates, All rights reserved.
Editor: Jane Guillette; Systems and Distribution: Colby Miers, Los Angeles