

CBO Reports on Projected Federal Health Spending, Sets Stage for Debt Ceiling, Appropriations Debates
CBO Reports on Projected Federal Health Spending, Sets Stage for Debt Ceiling, Appropriations Debates
DCMedical News is published every day both the House and the Senate are scheduled to be in session.
The Congressional Budget Office reported (here, health excerpts here) its projections in health and other federal areas of spending to the Republican Members of the House Energy and Commerce Committee.
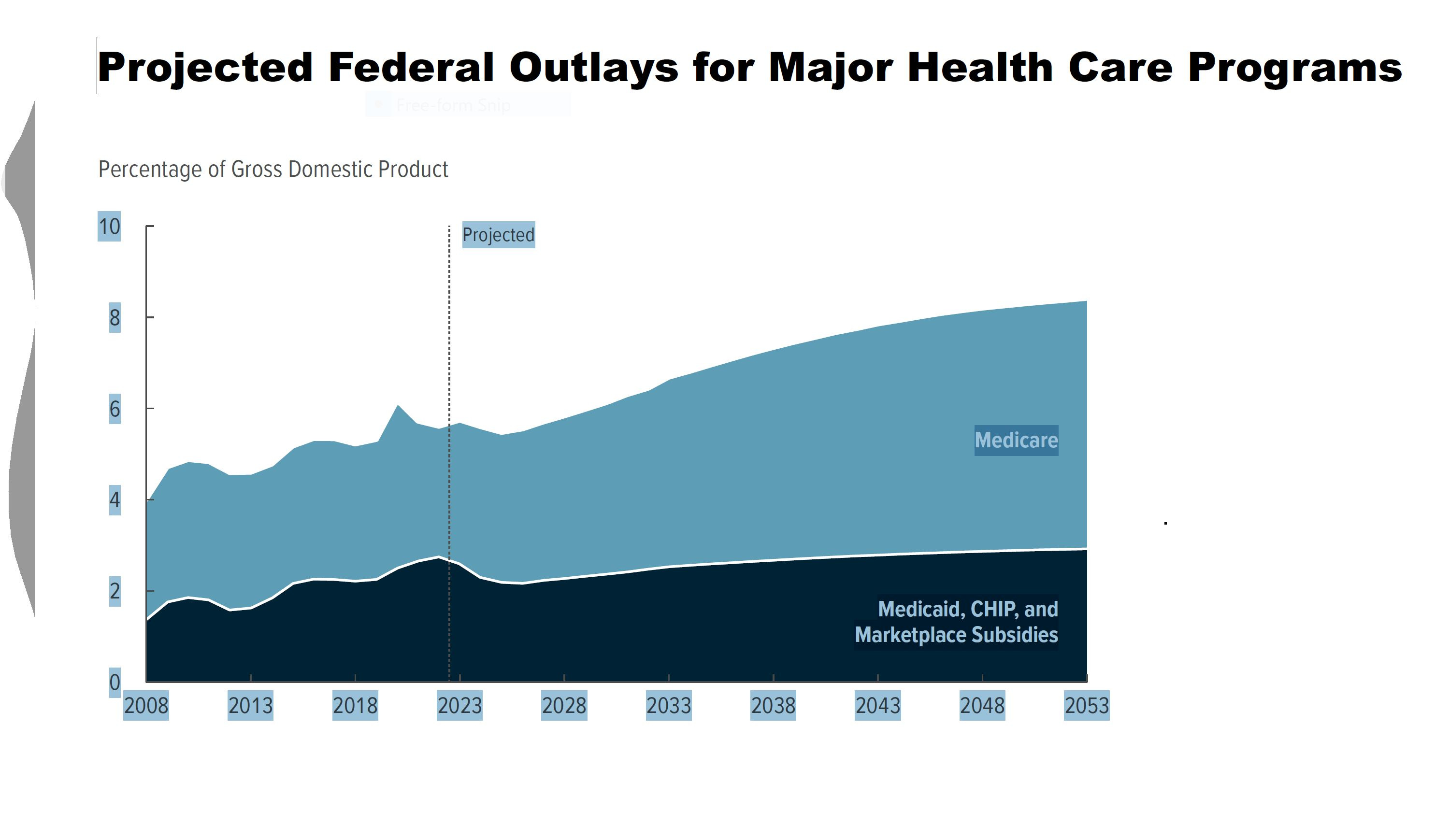
The report noted that “Projected mandatory spending for health totals $760 billion in 2023 and $9.1 trillion over the 2023–2033 period. Projected discretionary spending for health totals $110 billion in 2023 and $1.2 trillion over the 2023–2033 period if appropriations grow with inflation . . . Projected spending for Medicare totals $820 billion in 2023 and $13.1 trillion over the 2023–2033 period, almost all of which is mandatory.”
CBO suggested “Options for Larger Spending Reductions for Fiscal Years 2023 to 2032 That Relate to Health Care” including establishing caps on federal spending for Medicaid; limiting state taxes on health providers [which serve to increase the state “match” and therefore increase federal Medicaid matching funds]; reducing federal Medicaid matching rates; increasing Medicare part B premiums; reducing Medicare Advantage benchmarks; reducing tax subsidies for employer-paid health insurance; and reducing Social Security benefits for high earners.”
DOCTORS, NURSES AND OTHER HEALTH PROFESSIONALS
Medical Societies Attack Prior Authorization
A letter from one hundred medical organizations (here) to CMS noted that “American Medical Association (AMA) survey data show that 93 percent of physicians report care delays or disruptions associated with PA. AMA data also show that 34 percent of physicians report that PA has led to a serious adverse event (e.g., hospitalization, permanent impairment, or even death) for a patient in their care.”
They added, “Moreover, the Office of Inspector General (OIG) 2022 report found that 13 percent of PA requests denied by Medicare Advantage (MA) plans met Medicare coverage rules, and 18 percent of payment request denials met Medicare and MA billing rules.”
Is Auditing Overpayment to MA Plans the Same as “Cutting” Medicare Advantage?
A statement from The White House (here) weighs in on the representation that the Administration, in supporting audits of overpayments, and demanding repayments, is curtailing MA benefits to seniors. According to the statement, “Audits are unequivocally not cuts,” and “CMS is obligated under federal authorities to identify Medicare improper payments and to recover debts.”
The statement continues, “Due to growing enrollment, Medicare Advantage now represents about half of the Medicare program,” and “Medicare Advantage plans receive more than $420 billion in payments each year,” and cited “24 OIG reports [which] identify or estimate overpayments made to Medicare Advantage plans, as well as plan behavior that may have resulted in improper payments.”
Did 2021 Evaluation and Management Code Changes Shift Payment Amounts from Specialists to Primary Care Physicians?
Not much, according to a new study in JAMA (here). “The difference in the median total Medicare payments received by primary care physicians compared with specialists was $40,260 in July-December 2020 and $39,435 in July-December 2021 (a 2.0% decrease).”
HOSPITALS, NURSING HOMES AND OTHER HEALTH CARE FACILITIES
Diagnostic Error in the Emergency Department
Drs. Jonathan Edlow and Peter Provonost tackle (here) the long term meaning of the AHRQ study of ED error, a 744 page tome published in December, 2022. “Few will read the entire 744-page document. However, most will read the eye-catching finding: ‘With 130 million U.S. ED visits, estimated rates for diagnostic error (5.7%), misdiagnosis-related harms (2.0%), and serious misdiagnosis-related harms (0.3%) could translate to more than 7 million errors, 2.5 million harms, and 350 000 patients suffering potentially preventable permanent disability or death.’”
The authors note, “First, diagnostic errors are universal and implicate all specialties and areas of health care. The AHRQ report notes that diagnostic error rates estimated in the ED are remarkably similar to those in other areas of medicine. The report estimates a total ED diagnostic error rate of 5.7% and notes that other studies have found a 6.3% rate among primary care patients and roughly 8% in hospital autopsies . . . The error and harm rates cited for ED visits, primary care patients, and hospitalized patients are very similar, even though emergency clinicians see any and all patients, unscheduled, under great time pressure, often in an overcrowded, chaotic environment with frequent distractions.”
MEDICARE, MEDICAID AND COMMERCIAL HEALTH INSURANCE
Compromise Characterizes CMS Recovery of Risk Adjustment Over Payments From MA Plans
Health Affairs (here) carries a report of the decision by CMS to pursue wider scale risk adjustment audit corrections, but for fewer years (to 2018, not to 2011). “Risk adjustment is hugely important in Medicare Advantage (MA) . . . because insurers have considerable control over the documentation, it is common for insurers to erroneously document patient risk and receive inflated payments from the Centers for Medicare and Medicaid Services (CMS).”
The report continues, “Risk Adjustment Data Validation (RADV) audits are CMS’s primary means of policing risk adjustment. RADV audits seek to ensure the integrity of the MA program by identifying improper risk documentation among MA insurers . . . Auditors. . comb through each beneficiary’s medical records to determine whether diagnoses that the MA plan submitted are supported by documentation in the medical record. From this process, auditors can calculate an error rate for the sample, which can then be extrapolated to the rest of the contract. For instance, if auditors determine that an insurer over coded a sample’s risk by 5 percent, auditors could infer that plans under that contract were overpaid by 5 percent. Historically, however, CMS has only sought to collect the overpayments identified for the sample of audited beneficiaries.”
“On February 1, 2023, CMS published a long-awaited final rule that will shift the state of play in the RADV audit program by extrapolating the sample’s error rate to the entire contract, starting with program year (PY) 2018. Once it goes into effect on April 3, 2023, CMS estimates it will result in the recoupment of $4.7 billion in overpayments from MA insurers over the next decade.”
PUBLICATION SCHEDULE FOR DCMEDICAL NEWS
March 7, 8, 9, 22, 23, 24, 27, 28, 29, 30
April 17, 18, 19, 20, 25, 26, 27, 28
May 9, 10, 11, 12, 15, 16, 17, 18
Notes to Fred Hyde, MD, JD, MBA, news@dcmedicalnews.org
© 2023 Fred Hyde & Associates, All rights reserved.
Editor: Jane Guillette; Systems and Distribution: Colby Miers, Los Angeles